Sunday 12 April 2020

How do you begin to social distance in a hospital? (gpointstudio)
Let me say before I start, that I believe the UK’s National Health Service is doing astonishing things and its staff cannot be faulted for what they did, are doing and will do. If you doubt that for one moment, have a look at Boris Johnson’s thanks to those who rescued him from the jaws of possible death. But despite the efforts and unquestionable bravery of its staff, there are aspects of healthcare during this Covid Crisis that have me wondering.
In my defence I should say that I am a medic, that I am presently doing my bit for the Covid community and thereby putting myself, and my family, at risk. I am male, aged nearly 67 years, and am a dead ringer for Croak Corner when it comes to apportioning ventilators. In the eyes of a 40-year-old physician, who might handle the triage should I be admitted, I am simply not worth saving. As a surgeon, for that is what I am, I have spent my life keeping actions sterile so that I do not infect my patients. As a result, I have picked up a thing or two about avoiding contamination.
The other day, during a period of stay-at-homing, I found myself flicking through Oscar Wilde’s play, The Importance of Being Earnest. There, I came across the words of Lady Bracknell.
“To lose one parent, Mr Worthing,” she says, “may be regarded as misfortune; to lose both looks like carelessness.” Lady Bracknell had a point.
So far, many hundreds of healthcare workers worldwide have perished from Covid-19. Not all have been old and crumbly. Is this just misfortune or might healthcare have done better?
Even before the Covid-19 crisis began, the NHS was struggling. The British Medical Association stated quite recently, “The NHS is overstretched and underfunded, putting health services under unsustainable pressure.”
At the time, more was being spent on the NHS than ever before, with over 30% of the public services budget being dedicated to it. Yet key Accident and Emergency targets were being missed in the face of increasing demand, the country’s population was ageing, and care of the elderly was costing more.
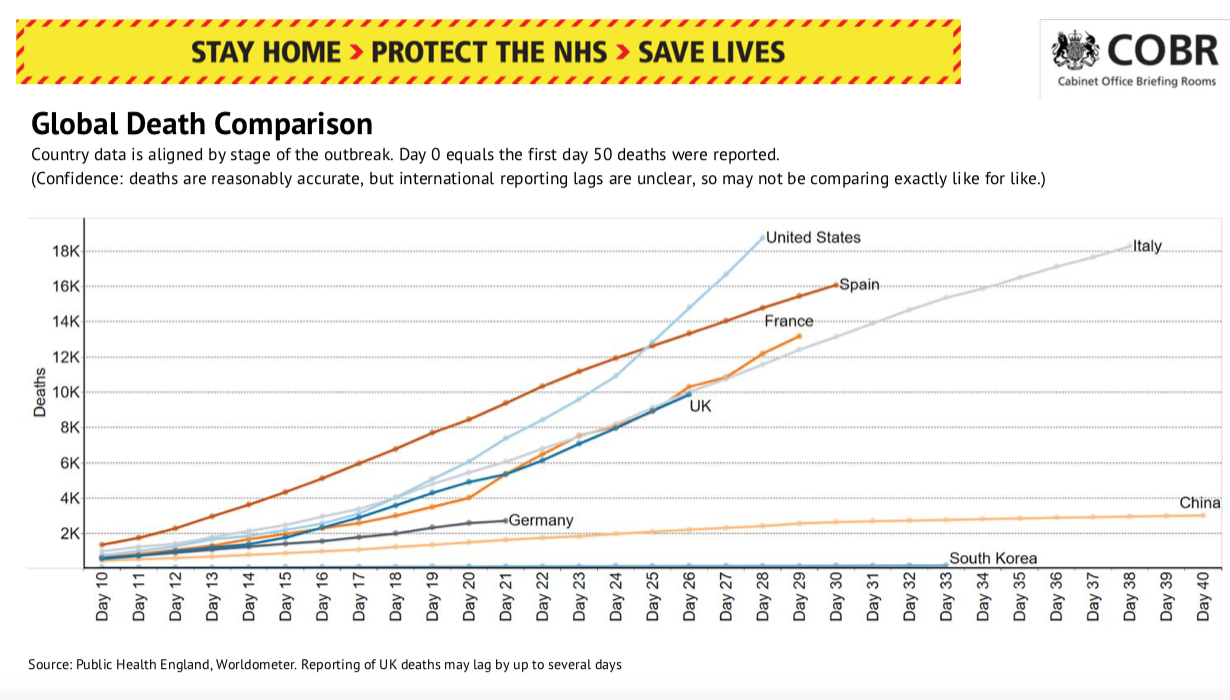
Germany leads the European field for success at the moment
The NHS costs roughly £140 billion to run each year, which is ten times the figure spent on it 60 years ago. As a percentage of GDP, this is less than so many others. Individual leading EU countries such as France and Germany spend significantly more on health than the UK. For example, in 2017 Germany spent 11.3% GDP on health, compared with the UK’s 9.7%.
Within this context of money, NHS Trusts employ 1.1 million whole-time equivalent (WTE) staff, the pay bill being its single biggest area of expenditure. Total pay costs are over £52 billion annually, a sum that includes a £1.5 billion overspend, most of which is spent on frontline staff for patient-related care. Like so many things in life, you get what you pay for. The more part-time staff you have, the less loyalty is created, and the harder it is to encourage new arrivals to adhere to local policies and procedures. That can include hand washing, social distancing, and plenty of other requirements, too.
When I hear from friends around the world that medical staff are dropping like pins – those are the words of an Italian – and that a number have now died, instantly I ask myself why. Is it all about the patient, or could there be other things afoot? Researchers have suggested that roughly 15% of Covid-19 cases are work-related, and of these, 22% are healthcare workers. Behind them come drivers and transport workers (18%), services and sales workers (18%), cleaning and domestic workers (9%), and public safety workers (7%).
Another report also intrigued me. It came from Singapore and described a single patient, a middle-aged man who was admitted with respiratory distress, but where Covid-19 was only diagnosed on his day of discharge. Panic ensued and the 41 healthcare workers who had been involved in his treatment were tracked down. Each had been exposed to aerosol-generating procedures for at least 10 minutes, and at a distance of less than two metres. Most had been wearing a simple surgical mask and gloves. A few had been wearing N95 masks. You know what? None of the workers developed Covid-19. That finding astonished me.
From my friends in other countries, and from my many colleagues in UK, most are saying the same thing. They are less worried by their journey to their hospital, even if it happens to be by public transport, than they are once they arrive.
One described a police guard outside the hospital’s front entrance. The four policemen narrowed the approach to less than one metre. When reminded, the police would step aside and let my colleague pass in safety, but that was an exception not a given.
Inside many hospitals, especially in historic cities, corridors are narrow. These are places that were not designed for social distancing when they were constructed. In a large teaching hospital, there can be 10,000 healthcare staff on duty at any one time. They will naturally congregate, outside in good weather or inside if bad. Shops and cafés in hospital concourses remain open and although distance markers may be etched on the floors, there are no such marks elsewhere in the building, so staff can do as they desire.
Because the buildings do not lend themselves to social distancing, at work staff can find it hard to keep apart, while outside they are obliged to do so. Meanwhile, the public for whom they care are expected to take full precautions at all times.
The commonest hospital-acquired infection is pneumonia (Dr_Microbe)
Hospital-acquired infections are a sad fact of life and existed even before the Covid Crisis. In the USA, the Centers for Disease Control and Prevention (CDC) once estimated that 1.7 million people were infected annually by hospital-acquired infections in the USA. These led to 99,000 deaths, of which roughly 36,000 were for pneumonia. In England alone, in 2011 there were said to be 300,000 patients each year who acquired a healthcare-associated infection, with pneumonia and lower respiratory tract infections being responsible for nearly 23% of them. One report estimated that each year, up to 5.2 million patients in European hospitals could suffer from a hospital-acquired infection. The European Centre for Disease Prevention and Control (ECDC) wrote in 2013 that on any given day in Europe, there are 80,000 patients with at least one hospital-acquired infection. Intensive care units are especially prone to them, with 19.5% of patients being affected. The most common infections are pneumonia (19.4%) and lower respiratory tract infections (4.1%).
It appears that hospitals can be pestilent places, and that was before Covid-19.
And PPE? Barely a press conference, newspaper or web site is without comment on Personal Protective Equipment these days. The nation is told that its lack is leading to a real and unnecessary risk exposure to the healthcare staff for whom it is designed. That is indeed a fact. Yet even with PPE, there is a trick in how it is used. That needs training and experience. It is not a matter of putting it on any old how and thereafter you will be safe. It is hot, uncomfortable and sweaty and is the last thing you would wear unless absolutely necessary.
PPE is largely worthless if you do not know how to use it. The highest risk of contamination is when doffing, which is taking it off. Even the non-healthcare mask-wearers I see walking London’s streets, and who might have invested in an upmarket fashion-house mask, may feel safe but, for a moment, think of the bugs. The outside of the mask will be crawling with them, whatever design of mask is chosen. The moment the wearer removes the mask barehanded, and then perhaps idly scratches their nose, Covid-19 is in there and will not be gone in a hurry. Apply that logic to a full house of PPE in a hospital healthcare worker, and you might understand the problem.
I thus worry that healthcare staff, however splendid their efforts, may be as much a hazard to each other as their patients are to them. No better example of this can there be than the Accident & Emergency Department of the Royal Gwent Hospital in Newport, where approximately half of the consultants and nursing staff have tested positive for the virus. My question is simple – did they acquire the disease from their patients, or did they give it to each other? And to how many others did they give the disease before they were able to self-isolate? Healthcare workers are an established source of infection, simply because of the life they lead.
Any amount of dedication cannot avoid that.