Wednesday 29 April 2020

Whenever I listen to the radio I become upset (SplitShire)
Some days, from the moment you wake up, you realise there will be problems. For me, it started at 0430hrs when I turned over in bed, rubbed my left eye, and poked it by mistake. The thing started watering, the pain was agonising, and two minutes’ later I was splashing cold water over my face in an attempt to relieve the discomfort. I got there in the end, although looked as if I had been crying all night, and so went for an early stagger-stumble through central London. I kept one eye closed and hoped no one would see me.
One dog-walker saw me approach, took a rapid look at my screwed-up face, and gathered up her unleashed pooch for protection. For me that was a eureka moment. Come the revolution, when walkers and stagger-stumblers extract their revenge against the nation’s joggers, cyclists and unleashed dog-walkers, one way to frighten the opposition is to look like a loonie. I achieved that this morning easily.
Asteroid 1998 is on its way to miss us
Apart from my eye, and in case there was any hope of relaxing, BBC Radio reminded me that fatalities in the USA have now surpassed those that took place over 20 years of Vietnam War, and that the true number of infections may be ten times what is known. Do I really want to hear that before breakfast? Just in case there is any chance I might feel happy, the BBC concluded by saying that an asteroid is presently deciding if it wants to hit Earth. Apparently, it is travelling at slightly less than 20,000 miles per hour, will pass within 4 million miles, is 1.2 miles wide and, they say, is “not expected” to collide with our planet. Of course, Covid-19 was “not expected” to become a pandemic, so I have no need to worry. After all, I have a red eye, am surrounded by a deadly virus, my American brothers are dropping like flies, and Armageddon is around the corner. What would anyone have to worry about?
My supermarket project at a nearby teaching hospital has been placed on hold for today and begins once again tomorrow, which is secretly good news. I am so far behind with my administration, I feel embarrassed, and could do with some time at my desk. Most of the communication for the supermarket project is through WhatsApp, which is fine, but I am all fingers and thumbs on a mobile screen, so must look to others as if I am illiterate. There are also three WhatsApp groups, each dealing with the same topic, so right now I am more than confused.
The care homes have also been in touch, seeking medical advice, as they do not know which way to turn when in trouble. Because of the closed nature of care homes, once the bug has got inside, it travels round the premises like wildfire. The general practitioners will often refuse to go into care homes these days, for fear they will infect the remainder of their patients. Plus, of course, a lack of the dreaded PPE, which has still not left the headlines. A cabinet minister has already stated that the early focus of the government was on the NHS and not care homes, which was a brave thing to say. At the moment, there may be more deaths taking place in care homes than hospitals, which to anyone must be unacceptable.
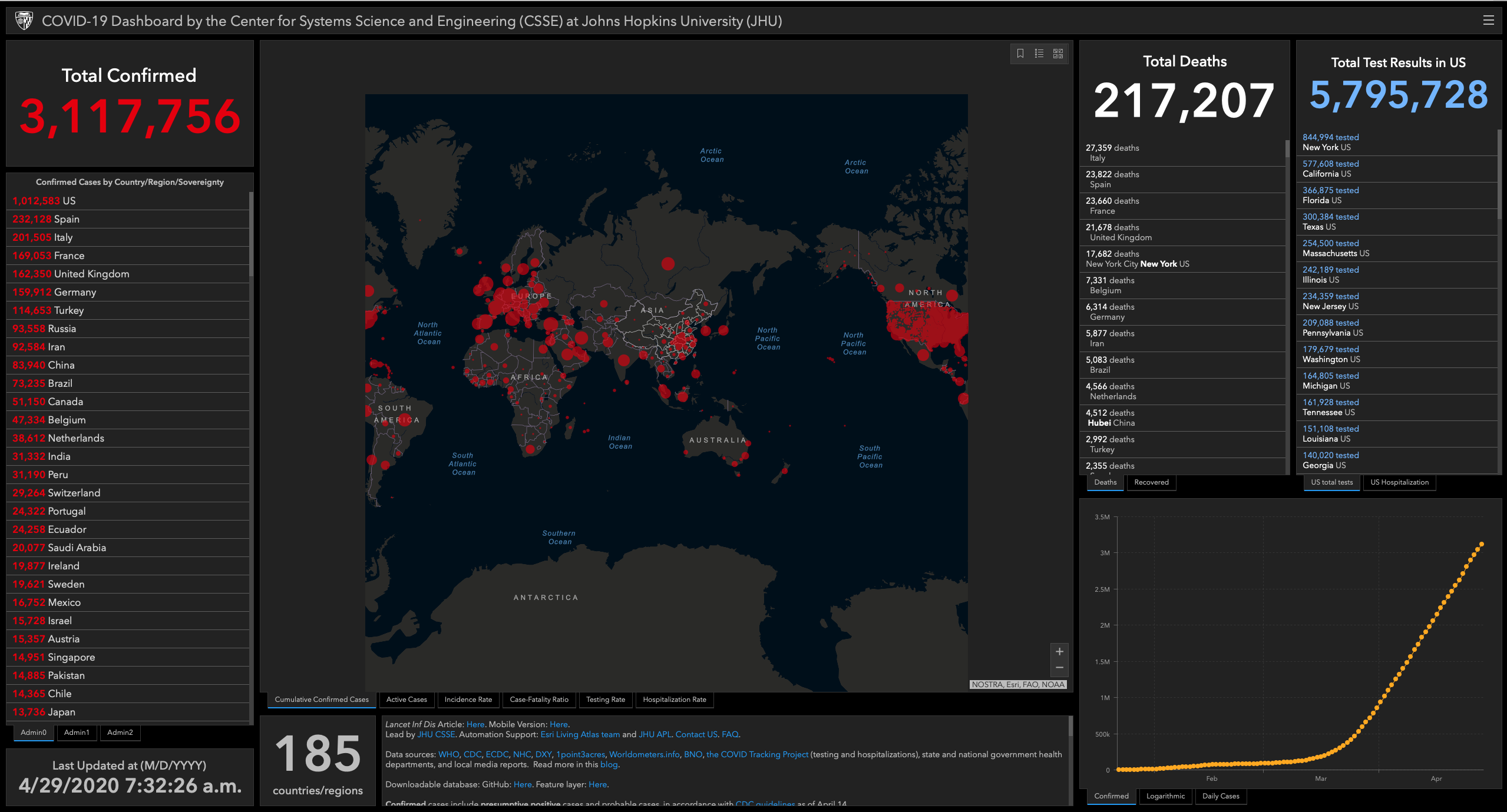
The situation this morning – 29 April 2020 (courtesy Center for Systems Science and Engineering at Johns Hopkins University)
My humanitarian work in the Middle East, which is where I spend much of my time as a surgeon these days, has unexpectedly reared its head. I thought they had stopped the war, but clearly not. I cannot travel there at the moment, but there are capable teams on the ground in the Middle East, although they are also in lockdown. However, when needs must they swing into action. There is a patient with a dislocated hip joint who is in trouble, so three of us – one from Canada, one from Italy, and me – have been looking at X-rays that have been emailed to us and discussing the various alternatives. Unusually for three surgeons, we appear to have agreed a common plan, so the patient is headed for a Middle East operating theatre in 36 hours’ time. I can only hope that what we have suggested works out safely. One thing is for certain, the patient cannot be left as he is and cannot wait for life to return to normal. Covid lockdowns worldwide affect many things, not just Covid.
I heard today that the UK aims to create infection-free hospitals. This would allow Covid-19 to be treated in one establishment and everything else in another. This is manifestly a good idea in principle, yet over many decades of medical work, I have still to find a hospital that is free from infection. Some are worse than others but nowhere is exempt. Hospital-acquired infections are a huge problem worldwide. In the USA, which you would have thought should be a beacon of perfect healthcare, even before Covid-19, one in 25 hospital patients had at least one infection associated with their care, or the hospital environment. As a surgeon, I have spent much of my life trying to avoid cross-infection between patients and staff. It is a significant part of my job. There is little purpose in denying its existence. After all, there is a Healthcare Infection Society, journals, meetings, conferences, guidelines, you name them. Hospital-acquired infection is an undesirable fact of life.
Some hospitals, University College Hospital in London is an example, have started to test their own staff for Covid-19 already. This is not before time as I will wager, when the dust eventually settles, healthcare staff will be seen as one of the biggest sources of infection, certainly for each other and possibly of their patients. No wonder the public is fearful of going to hospitals right now. Professor Charles Swanton, head of the Francis Crick Institute’s testing facility said it in one, when he was quoted in The Guardian:

Professor Charles Swanton who believes healthcare workers should be screened (Crick Institute)
“It’s almost untenable to argue you shouldn’t be screening and isolating healthcare workers.”
Well done, Professor Swanton, for saying what so many others think.
As I look forward to a likely second wave, something I cannot see the UK avoiding, I note that NHS England has recently issued an alert over rising symptoms in children, who need admission to intensive care. The symptoms, which have been seen in London and other parts of the UK, have been described as a multi-system inflammatory state, added to features of what is called toxic shock syndrome and atypical Kawasaki disease. The blood parameters are consistent with severe Covid-19. Toxic shock syndrome as an acute life-threatening illness, usually precipitated by infection. Kawasaki disease is an acute febrile illness of early childhood associated with inflammation of the medium-sized arteries. Take the two together and a patient has a problem.
At the moment there is only a handful of cases, but I worry that a second wave may start to involve a different age range of patient, which might imply mutation. Second waves have often been worse than first waves and may also affect different portions of the population. The medics have done well to spot the problem so early. Fingers crossed it is a chance finding and nothing to do with the pandemic that surrounds us, but only time will tell.
I am disposable, the younger ones are not. The last thing we need right now is a viral mutation.